Understanding the 4 Phases of the Female Hormone Cycle
A Complete 28-Day Guide to the Endocrine Rhythm
The female body does not operate in isolation from its hormones. In fact, nearly every shift in mood, energy, metabolism, and fertility is tied to a carefully timed hormonal rhythm that unfolds across roughly 28 days.
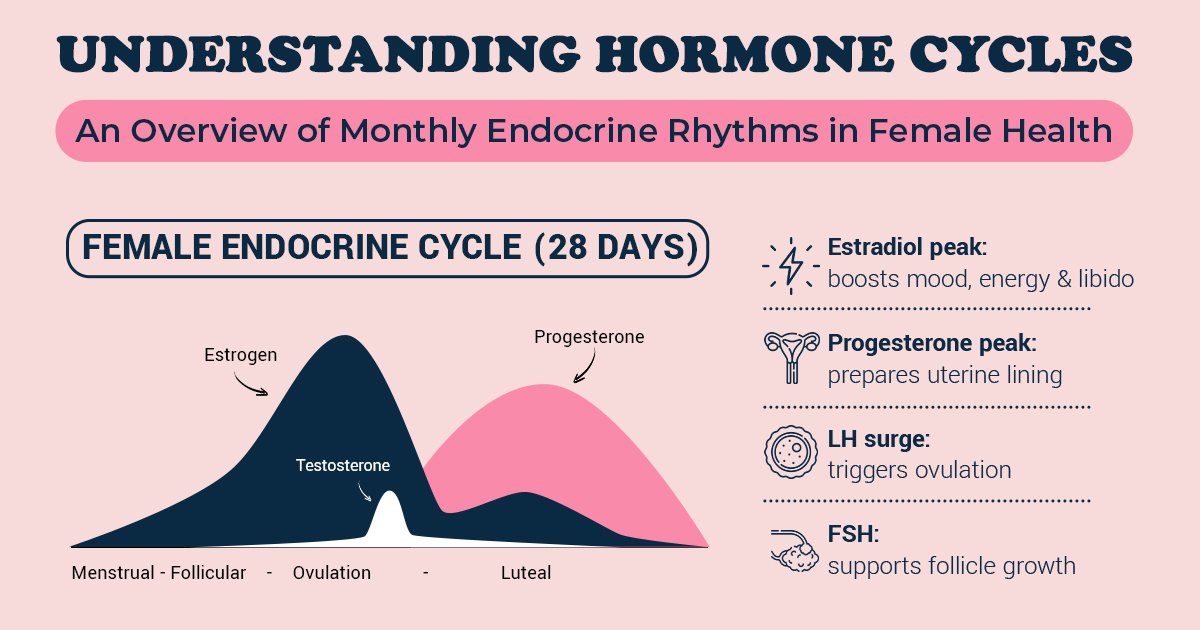
This rhythm is not random. It is orchestrated by the brain, the ovaries, and a delicate feedback loop between hormones such as estrogen, progesterone, luteinizing hormone (LH), and follicle-stimulating hormone (FSH). When working in harmony, this endocrine cycle supports ovulation, prepares the uterus for pregnancy, and then resets itself with remarkable precision.
Although cycle length can normally range from 21 to 35 days, the 28-day model helps illustrate the four distinct phases that define the female reproductive cycle: the menstrual phase, the follicular phase, ovulation, and the luteal phase.
Understanding each phase offers more than fertility awareness — it offers insight into overall health.
Phase 1: The Menstrual Phase — Reset and Renewal (Day 1–5)
The cycle begins on the first day of menstrual bleeding. At this point, both estrogen and progesterone levels have fallen significantly because pregnancy did not occur in the previous cycle. That hormonal drop is what signals the uterus to shed its lining.
This shedding is not just a surface event. The uterine lining, which had thickened in preparation for a potential embryo, breaks down and exits the body. During this time, inflammatory compounds called prostaglandins are released, which can contribute to cramping or lower abdominal discomfort.
While bleeding occurs, the brain is already preparing for the next cycle. FSH begins to rise subtly, stimulating the ovaries to recruit a new group of follicles. Each follicle contains an immature egg, and although several begin developing, typically only one will become dominant.
Because estrogen levels are at their lowest during menstruation, many women report lower energy, increased need for rest, and sometimes mental fog. This is physiologically understandable — estrogen has stimulating and mood-supporting effects, so its temporary decline can create a natural inward shift.
Rather than seeing this phase as weakness, it can be understood as biological recalibration.
Phase 2: The Follicular Phase — Growth and Rising Energy (Day 1–13)
The follicular phase technically begins on the first day of menstruation, but its most noticeable effects occur after bleeding ends.
As FSH continues stimulating follicle growth in the ovaries, the dominant follicle begins producing increasing amounts of estradiol, the most active form of estrogen. Estrogen does far more than support reproduction. It enhances blood flow, improves insulin sensitivity, sharpens cognitive function, and contributes to emotional resilience.
As estrogen rises through the mid-follicular days, the uterine lining begins rebuilding itself. Cells proliferate rapidly, forming a thickened endometrium capable of supporting implantation if pregnancy occurs.
By the late follicular phase, estrogen levels peak dramatically. This rise influences cervical mucus, making it clearer and more elastic — a biological adaptation designed to support sperm survival and mobility.
Many women notice improved concentration, stronger communication skills, and increased physical stamina during this phase. From a hormonal standpoint, this makes sense: estrogen enhances neurotransmitter activity, including serotonin and dopamine, which are closely linked to motivation and mood.
The body is not just preparing for ovulation — it is building toward it.
Phase 3: Ovulation — The Hormonal Surge (Around Day 14)
Ovulation is the shortest but most hormonally dynamic phase of the cycle.
When estrogen reaches a certain threshold, it sends a signal to the hypothalamus and pituitary gland in the brain. In response, the pituitary releases a sharp surge of LH. This LH surge is the critical trigger that causes the dominant follicle to release its mature egg.
Ovulation typically occurs 24 to 36 hours after the LH surge begins. The egg then travels into the fallopian tube, where it remains viable for about 12 to 24 hours. However, because sperm can survive inside the female reproductive tract for up to five days, the fertile window extends beyond ovulation itself.
Estrogen is still high around ovulation, which explains why many women feel socially confident, energized, and more sexually receptive at this time. There may also be subtle physical signs, such as mild pelvic sensation or a slight rise in basal body temperature after ovulation has occurred.
From a biological perspective, this is the moment of peak reproductive potential.
Phase 4: The Luteal Phase — Stabilization and Preparation (Day 15–28)
Once the egg is released, the follicle transforms into a structure known as the corpus luteum. Its primary function is to produce progesterone.
Progesterone shifts the body into a stabilizing mode. While estrogen promotes growth, progesterone promotes maintenance. It strengthens and stabilizes the uterine lining, making it receptive to implantation if fertilization occurs.
This hormone also has systemic effects. It slightly raises basal body temperature, influences the calming neurotransmitter GABA in the brain, and can slow digestive motility. These changes explain why some women feel calmer, warmer, or occasionally bloated during this phase.
If fertilization and implantation occur, progesterone remains elevated to support early pregnancy. If not, the corpus luteum gradually breaks down. Progesterone and estrogen levels decline, removing hormonal support for the uterine lining. That decline triggers menstruation — and the cycle begins again.
The luteal phase typically lasts between 12 and 14 days. A consistently short luteal phase may impact implantation potential, which is why it is often evaluated in fertility assessments.
The Bigger Endocrine Picture
The menstrual cycle is not just a reproductive event. It is a monthly indicator of endocrine health.
Estrogen influences bone density, cardiovascular health, skin integrity, and cognitive function. Progesterone plays a role in neurological balance and uterine stability. LH and FSH reflect communication between the brain and ovaries. When this communication is disrupted — due to stress, thyroid imbalance, PCOS, or metabolic dysfunction — the cycle often becomes irregular before other symptoms appear.
In this way, the menstrual cycle serves as a vital sign. Its regularity, duration, and symptom pattern offer insight into the broader hormonal ecosystem of the body.
Understanding these four phases transforms the way we interpret hormonal changes. Instead of seeing them as unpredictable fluctuations, we begin to recognize a structured rhythm — one that supports renewal, growth, release, and restoration every single month.
When that rhythm is respected and supported, it becomes one of the most reliable indicators of female health.